Colorectal cancer
If you or someone you love has just learned that colorectal cancer is a possibility, the flood of new terms and decisions can feel overwhelming. This guide explains, in plain and compassionate language, what colorectal cancer is, how it is found and staged, and the treatment options available today, drawing only on recognised cancer authorities. It is here to help you ask good questions and make informed choices, not to replace the personalised advice of a qualified oncology team.
What colorectal cancer is
Colorectal cancer is a cancer that begins in the large intestine, the final part of the digestive tract. The first several feet of the large intestine make up the colon, and the last few inches form the rectum, which connects to the anus. Cancer that starts in the colon is called colon cancer; cancer that starts in the rectum is called rectal cancer. Because the two share many features, they are often grouped together under the term colorectal cancer. You may also hear it called bowel cancer, particularly in the United Kingdom.
Most colorectal cancers begin as a small, non-cancerous growth on the inner lining of the colon or rectum called a polyp. Some polyps, especially a type known as an adenoma, can slowly change into cancer over a number of years. This slow progression is one reason screening can be effective: removing polyps before they turn cancerous can help prevent the disease, and finding cancer early tends to make it more treatable.
Colorectal cancer is among the most commonly diagnosed cancers. According to U.S. SEER data from the National Cancer Institute, it is one of the most common cancers and, in the United States, the second leading cause of cancer death when figures for men and women are combined. Overall rates in older adults have been falling in recent decades, an improvement often attributed in part to screening, while rates among some younger adults have been rising, which is changing how doctors think about who should be checked and when.
Colon cancer and rectal cancer: types and subtypes
Although colon and rectal cancer are closely related, their location matters. The rectum sits in a tight space within the pelvis, surrounded by other organs, which affects both surgery and whether radiotherapy is used. Colon cancer, higher up in the abdomen, is treated somewhat differently. This is why your care team will be precise about exactly where the tumour is.
The great majority of colorectal cancers, around nine in ten, are adenocarcinomas, which arise from the gland cells that line the inside of the colon and rectum. Within adenocarcinoma there are less common variants, such as mucinous and signet-ring cell types, which behave a little differently and which a pathologist identifies under the microscope.
Other, much rarer tumours can also develop in this part of the body, including neuroendocrine tumours, gastrointestinal stromal tumours (GISTs), lymphomas, and squamous cell carcinomas. Each of these is managed differently from typical adenocarcinoma, so an accurate diagnosis from a specialist pathologist is an essential first step.
Increasingly, doctors also describe a tumour by its molecular subtype, the specific genetic changes inside the cancer cells. Features such as mismatch repair (MMR) status, microsatellite instability (MSI), and mutations in genes including KRAS, NRAS, and BRAF are now central to choosing treatment, as described later in this guide.
Risk factors and causes
Colorectal cancer develops from a combination of factors, and having one or more does not mean you will develop the disease. The American Cancer Society divides risk factors into those you can change and those you cannot.
Factors you may be able to change include excess body weight, a diet high in red meat (such as beef, pork, and lamb) and processed meats (such as sausages and deli meats), heavy alcohol use, and smoking. Type 2 diabetes is also associated with higher risk. According to the American Cancer Society, more than half of all colorectal cancers are linked to risk factors that can be changed, which is why lifestyle choices and screening together can play a meaningful role.
Factors you cannot change include increasing age, a personal history of adenomatous polyps or earlier colorectal cancer, and a personal history of inflammatory bowel disease (ulcerative colitis or Crohn's disease), which can inflame the bowel lining over many years. Previous radiotherapy to the abdomen or pelvis can also raise risk. Risk also varies by racial and ethnic background.
Family history and inherited syndromes are important. According to the American Cancer Society, as many as one in three people who develop colorectal cancer have other family members who have had it, and about 5% have an inherited gene change. The most common inherited syndrome is Lynch syndrome (also called hereditary non-polyposis colorectal cancer), caused by changes in mismatch repair genes, which carries an increased lifetime risk and is linked to other cancers. Familial adenomatous polyposis (FAP), caused by changes in the APC gene, leads to large numbers of polyps and a high risk if untreated. If colorectal or related cancers run in your family, especially at a young age, ask about genetic counselling.
Signs and symptoms, and when to see a doctor
In its early stages colorectal cancer often causes no symptoms at all, which is one reason screening matters. When symptoms do appear, they can also be caused by far more common and harmless conditions such as haemorrhoids, infections, or irritable bowel syndrome. The point of seeing a doctor is not to assume the worst, but to have the cause identified and treated.
According to the American Cancer Society and the NHS, bowel cancer symptoms to be aware of include:
- A lasting change in bowel habits, such as diarrhoea, constipation, or narrowing of the stool, that continues for more than a few days
- Blood in or on the stool, which may be bright red, or stools that appear dark or black
- Bleeding from the back passage
- A persistent feeling that you need to empty your bowel that is not relieved by going
- Abdominal cramping, pain, or bloating
- Unintended weight loss
- Persistent tiredness or weakness, sometimes from anaemia caused by slow blood loss
The NHS advises seeing a GP if you have any of these symptoms for three weeks or more. Seek urgent medical advice if your stool is black or dark red, or if you have bloody diarrhoea, and seek emergency care if you are bleeding non-stop from the back passage. Early evaluation gives you the widest range of options if treatment turns out to be needed.
Screening and early detection
Colorectal cancer is one of the cancers that can sometimes be prevented through screening, because removing polyps can stop them from becoming cancer. Screening can also find cancer early, when it tends to be most treatable.
The American Cancer Society recommends that people at average risk begin regular screening at age 45, continuing through to at least age 75 for those in good health with a life expectancy greater than 10 years, with decisions for ages 76 to 85 made individually with a doctor. Several screening methods are considered acceptable, and the best test is often the one you will actually complete:
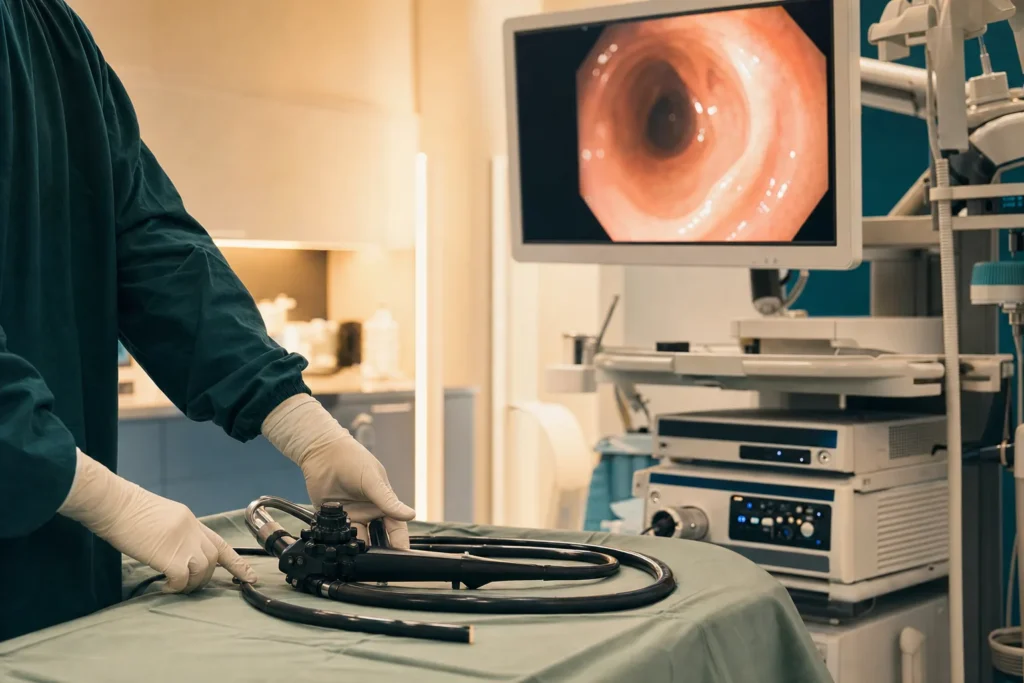
- Colonoscopy every 10 years, during which a doctor uses a thin, flexible camera to examine the entire colon and rectum and can remove polyps in the same session
- Stool-based tests, including the faecal immunochemical test (FIT) each year, the high-sensitivity guaiac-based faecal occult blood test each year, or a multi-target stool DNA test every three years
- Other visual exams such as flexible sigmoidoscopy every five years or CT colonography every five years
An important rule applies to all non-colonoscopy tests: any positive result should be followed up promptly with a colonoscopy. People with a strong family history, an inherited syndrome, inflammatory bowel disease, or other higher-risk features may need to start earlier and be screened more often. Discuss the right schedule with your doctor.
Diagnosis and staging
If symptoms or a screening test raise concern, the key diagnostic step is usually a colonoscopy with biopsy. The colonoscope lets the doctor see the lining of the bowel directly, and a small tissue sample (biopsy) is taken from any suspicious area. A pathologist then examines this tissue under a microscope; this is the way cancer is confirmed.
If cancer is confirmed, further tests determine how far it has spread, a process called staging. These commonly include CT scans of the chest, abdomen, and pelvis, and for rectal cancer a pelvic MRI to assess the tumour and nearby structures in detail. A blood test for a marker called CEA (carcinoembryonic antigen) may be used as a baseline and to monitor over time. The tumour tissue is also tested for biomarkers such as MMR/MSI status and mutations in KRAS, NRAS, and BRAF, which guide treatment choices.
Staging uses the American Joint Committee on Cancer (AJCC) TNM system, which considers how deeply the Tumour has grown into the bowel wall, whether nearby lymph Nodes contain cancer, and whether the cancer has spread, or Metastasised, to distant organs. These combine into stages 0 to IV:
- Stage 0: abnormal cells only in the innermost lining
- Stage I: cancer has grown into deeper layers of the wall but not into lymph nodes
- Stage II: cancer has grown through the wall but has not reached lymph nodes
- Stage III: cancer has spread to nearby lymph nodes but not to distant organs
- Stage IV: cancer has spread to distant organs such as the liver or lungs
Knowing the colorectal cancer stages helps your team recommend the most appropriate treatment, but staging is only one part of a fuller picture that also includes your overall health and the tumour's biology.
Treatment options
Modern colorectal cancer care is delivered by a multidisciplinary team, often discussed at a tumour board where surgeons, medical oncologists, radiation oncologists, radiologists, and pathologists agree on a plan together. Treatment is tailored to the cancer's location, stage, and molecular features, and to you as a person. The main approaches are used alone or in combination.
Surgery is a central treatment for cancer that has not spread to distant organs. Very early cancers or polyps may be removed during colonoscopy (polypectomy) or by local excision. More commonly, the surgeon removes the affected segment of bowel along with nearby lymph nodes and reconnects the healthy ends, a procedure called resection with anastomosis. Many operations can be performed using minimally invasive (laparoscopic or robotic) techniques through small incisions, which may mean less pain and a quicker recovery for suitable patients. In some cases, particularly with the rectum, a temporary or permanent stoma (an opening on the abdomen) is needed; a stoma care nurse helps you adjust.
Chemotherapy uses drugs such as fluorouracil, capecitabine, oxaliplatin, and irinotecan. It may be given after surgery (adjuvant) to lower the chance of recurrence in higher-risk colon cancers, before surgery to shrink a tumour, or as part of treatment for advanced disease.
Radiotherapy plays a particular role in rectal cancer, where it is often combined with chemotherapy before surgery to shrink the tumour and reduce the risk of it returning in the pelvis. It is used much less often for colon cancer.
Targeted therapy acts on specific features of cancer cells. Drugs that block tumour blood-vessel growth, and drugs in the anti-EGFR class (used when the tumour is RAS wild-type), are options mainly in advanced disease, guided by biomarker results. Immunotherapy with immune checkpoint inhibitors can be effective for tumours that are mismatch-repair-deficient or microsatellite instability-high (dMMR/MSI-H), which is why MSI testing is so important. Drug classes mentioned anywhere in this guide are neutral examples only; your oncologist will recommend specific medicines for your situation.
Prognosis and survival
Survival statistics can help you understand the disease in general terms, but they describe large groups of people and are not a prediction for any one individual. They are based on patients treated in the past, often before the newest therapies, and they cannot account for your particular tumour, your overall health, or how you respond to treatment. Please read the numbers below as context, and discuss what they mean for you with your own oncologist.
Using U.S. SEER data for 2016 to 2022, the National Cancer Institute reports an overall five-year relative survival of about 65% for colorectal cancer. Survival is strongly stage-dependent. SEER groups cases by how far the cancer has spread:
- Localised disease (confined to the bowel): about 91%
- Regional disease (spread to nearby lymph nodes): about 75%
- Distant disease (spread to other organs): about 17%
Two general points stand out. First, outcomes at the population level tend to be better when the cancer is found early, which is part of the rationale for screening and prompt evaluation of symptoms. Second, advanced colorectal cancer is still treatable, and treatments continue to develop; for some people with limited spread to the liver or lungs, for example, treatment may aim at long-term control. These figures set a general backdrop only, and your care team can speak to your specific circumstances.
Supportive and follow-up care
Treatment is about more than the cancer itself; it is about helping you live as well as possible throughout. Supportive (palliative) care, which can be provided alongside treatment at any stage, focuses on relieving symptoms and side effects such as pain, nausea, fatigue, and bowel changes, and on emotional and practical support for you and your family. Asking for this care early is a sign of good planning, not of giving up.
If you have a stoma, specialist stoma nurses provide hands-on training and ongoing support, and many people return to their normal activities over time. Dietitians can help with eating well during and after treatment, and counselling or peer support can help with the understandable anxiety that a cancer diagnosis brings.
After treatment, your team will arrange follow-up care to watch for any signs the cancer has returned and to manage long-term effects. This typically includes scheduled clinic visits, physical examinations, CEA blood tests, periodic imaging, and a surveillance colonoscopy programme. Keeping to your follow-up schedule is one of the most valuable things you can do, because recurrences found early are often more treatable.
Planning treatment abroad: what affects cost and how to prepare your records
Some patients and families consider receiving care in another country, whether to access a particular team, to reduce waiting times, or for personal reasons. If you are weighing treatment abroad, it helps to understand what shapes the overall cost and effort, so you can plan realistically and request a tailored estimate rather than relying on a single headline figure.
The factors that most influence cost and complexity include the type and stage of your cancer, the specific treatments needed (for example surgery alone versus surgery combined with chemotherapy, radiotherapy, or targeted and immune therapies), the surgical approach (such as minimally invasive versus open surgery), the length of any hospital stay, the laboratory and biomarker testing required, and the imaging and follow-up scans involved. Travel, accommodation, interpreting services, and the duration of your stay also add up.
To prepare, gather your medical records in one place: pathology and biopsy reports, all imaging (CT and MRI scans on disc or in digital form) with the radiology reports, your colonoscopy report, recent blood tests including CEA, biomarker results (MMR/MSI and RAS/BRAF status if done), a summary of any treatment you have already received, and a current medication list. Having these ready allows a specialist team to review your case accurately and give you a clear, personalised estimate through a consultation. BergemHealth can help coordinate this review and translate your records as needed.
Considering Turkiye and choosing a cancer centre
Turkiye (Turkey) has become an established destination for international patients seeking cancer care, with hospitals that offer modern surgical facilities, radiotherapy, and access to systemic therapies, often with dedicated international patient services. Whatever country or hospital you are considering, the priority is the quality and coordination of the team that will treat you, rather than any single feature.
When evaluating a cancer centre, it is reasonable to verify the following:
- That care is delivered by a genuine multidisciplinary team and that your case will be reviewed at a tumour board where surgeons, oncologists, radiologists, and pathologists plan together
- The hospital's accreditation and the qualifications and experience of the specific surgeons and oncologists involved
- The availability of the full range of treatments you may need, including minimally invasive surgery, radiotherapy for rectal cancer, and biomarker-guided targeted and immune therapies
- Access to modern pathology and molecular testing, since accurate diagnosis and biomarker results drive treatment
- Clear arrangements for follow-up, communication with your doctors at home, language support, and a written treatment and cost plan before you commit
A trustworthy team will welcome your questions, encourage a second opinion, and never pressure you. As a medical-tourism concierge, BergemHealth's role is to help you find and coordinate appropriate care and to ensure your records and questions reach the right specialists.
Clinical trials and second opinions
Clinical trials study new ways to prevent, detect, and treat cancer, and they are how today's standard treatments came to exist. For some patients, a trial offers access to approaches not yet widely available, always with careful monitoring. Trials are entirely voluntary, and you can ask your oncologist whether any are appropriate for your stage and tumour biology, or consult the National Cancer Institute's trial resources.
Seeking a second opinion is a normal and respected part of cancer care, not a sign of distrust. Because colorectal cancer treatment depends heavily on accurate staging and biomarker results, a fresh review by another specialist team can confirm the plan or suggest alternatives, and many people find it brings peace of mind. Whatever you decide, take the time you need, lean on your multidisciplinary team, and make the choice that is right for you.
Frequently asked questions
What is the difference between colon cancer and rectal cancer?
What are the early warning symptoms of bowel cancer?
At what age should screening for colorectal cancer start?
Is a colonoscopy the only way to screen for colorectal cancer?
What do the colorectal cancer stages mean?
How is colorectal cancer treated?
Why does MSI or biomarker testing matter?
Can colorectal cancer be cured?
Should I get a second opinion?
How do I prepare my records for treatment abroad?
This article is for general information only and is not medical advice. Always consult a qualified doctor about your individual case.
Considering this procedure?
Send us your photos and questions. A BergemHealth coordinator and a department-head specialist will review your case and reply with honest, personalised guidance — no obligation.
Free consultation