Heart failure
Heart failure sounds frightening, but the name does not mean the heart has stopped. It means the heart is not pumping blood as well as it should, so the body has to work harder. With modern medicines, devices and lifestyle support, many people live for years with their symptoms well controlled. This guide explains, in plain language, what heart failure is, how doctors find and treat it, and how to plan care calmly if you are considering treatment abroad.
What heart failure is
Heart failure is a long-term condition in which the heart cannot pump blood around the body as well as it should. It does not mean the heart has stopped or is about to stop. It simply means the heart muscle has become too weak or too stiff to keep up with the body's demands, so blood and fluid can build up and organs may not get all the oxygen they need.
Doctors sometimes call it congestive heart failure, because fluid can collect (or "congest") in the lungs, legs and feet. The word "failure" here is medical shorthand, not a description of how serious your day will be. Many people with heart failure work, travel and enjoy life with the right treatment.
To understand it, it helps to picture the heart as a pump with four chambers. With each beat, the lower chambers (the ventricles) squeeze blood out to the lungs and the rest of the body, then relax to fill again. In heart failure, either the squeeze is too weak, or the muscle is too stiff to fill properly, or both. Over time this can cause breathlessness, tiredness and swelling.
Heart failure is common, especially after the age of 65, and it usually develops gradually. Because it tends to be a lasting condition, the goal of treatment is to ease symptoms, slow its progression and keep you feeling as well as possible for as long as possible.
Types and subtypes
Doctors describe heart failure in a few different ways, depending on which part of the heart is affected and how well it pumps.
By side of the heart:
- Left-sided heart failure is the most common. The left side pumps oxygen-rich blood to the body. When it struggles, fluid can back up into the lungs, causing breathlessness.
- Right-sided heart failure often follows left-sided failure. The right side sends blood to the lungs; when it weakens, fluid can build up in the legs, ankles and abdomen.
- Biventricular heart failure means both sides are affected.
By ejection fraction. Ejection fraction (EF) is the percentage of blood the main pumping chamber squeezes out with each beat. It is one of the most important numbers in heart failure. Based on guidelines from the European Society of Cardiology, doctors group it as:
- Reduced EF (HFrEF): ejection fraction of 40% or less. The pump is weakened.
- Mildly reduced EF (HFmrEF): 41% to 49%.
- Preserved EF (HFpEF): 50% or higher. Here the squeeze looks normal, but the heart muscle is stiff and does not fill well.
A rare form called high-output heart failure happens when the heart pumps normally but the body demands more blood than it can supply, for example with severe anaemia or an overactive thyroid.
Causes and risk factors
Heart failure is usually the end result of something that has strained or damaged the heart over time, rather than a single sudden event.
Common underlying causes include:
- Coronary artery disease (narrowed heart arteries) and previous heart attacks, which can damage the heart muscle.
- High blood pressure (hypertension), which makes the heart work harder for years.
- Cardiomyopathy — diseases of the heart muscle itself, sometimes inherited.
- Heart valve problems and congenital heart disease (a heart difference present from birth).
- Abnormal heart rhythms (arrhythmias), such as atrial fibrillation.
Things that raise the risk of developing heart failure include being over 65, diabetes, obesity, smoking, drinking too much alcohol, a high-salt diet, a sedentary lifestyle, an overactive thyroid, and certain infections or medicines that can affect the heart. A family history of cardiomyopathy can also play a part. According to MedlinePlus, people of African American background may be at higher risk in some populations.
Many of these risk factors can be improved, which is why managing blood pressure, diabetes and weight matters so much both for preventing heart failure and for living well with it.
Signs and symptoms (and when to see a doctor)
The most common symptoms of heart failure are caused by fluid building up and by the body not getting enough oxygen-rich blood.
- Breathlessness — at first during activity, later sometimes at rest or when lying flat.
- Tiredness and weakness that does not improve with rest.
- Swelling in the ankles, legs, feet or abdomen.
- Rapid or unexpected weight gain from fluid retention.
- A persistent cough or wheeze, sometimes worse at night.
- Needing to urinate more often at night, fast or irregular heartbeats, dizziness, reduced appetite or nausea.
Symptoms can be mild at first and easy to put down to ageing or being unfit, so it is worth paying attention if they persist or slowly worsen.
See your doctor if you have ongoing or worsening breathlessness, tiredness or swelling. Seek emergency care (call your local emergency number) for sudden severe breathlessness, chest pain, fainting, or a fast irregular heartbeat with breathlessness — these need urgent assessment. Sudden weight gain over a day or two can signal fluid build-up and should be reported promptly.
Screening and early detection
There is no single routine screening test for heart failure offered to the general public the way there is for some cancers. Instead, early detection relies on managing and monitoring the conditions that lead to it.
If you have high blood pressure, diabetes, coronary artery disease, or a family history of heart muscle disease, regular check-ups are the most useful form of early detection. Your doctor can keep an eye on your blood pressure, cholesterol, blood sugar and weight, and act early if your heart shows signs of strain.
The American College of Cardiology and American Heart Association describe a "Stage A" — people who are at risk of heart failure but have no symptoms and no structural heart damage yet. Identifying and treating risk factors at this stage is the closest thing to screening, and it can genuinely delay or prevent heart failure from developing.
If symptoms do appear, a blood test for natriuretic peptides (BNP or NT-proBNP) can help flag heart failure early and prompt further tests. Tell your doctor about any new breathlessness, swelling or unusual tiredness rather than waiting.
How heart failure is diagnosed
Diagnosing heart failure starts with a conversation about your symptoms and medical history, followed by a physical examination in which the doctor listens to your heart and lungs and checks for swelling.
Common tests include:
- Blood tests, including BNP or NT-proBNP — natural substances the heart releases when it is under strain. Raised levels support the diagnosis. Other blood tests check kidney, thyroid and blood-count problems that can mimic or worsen heart failure.
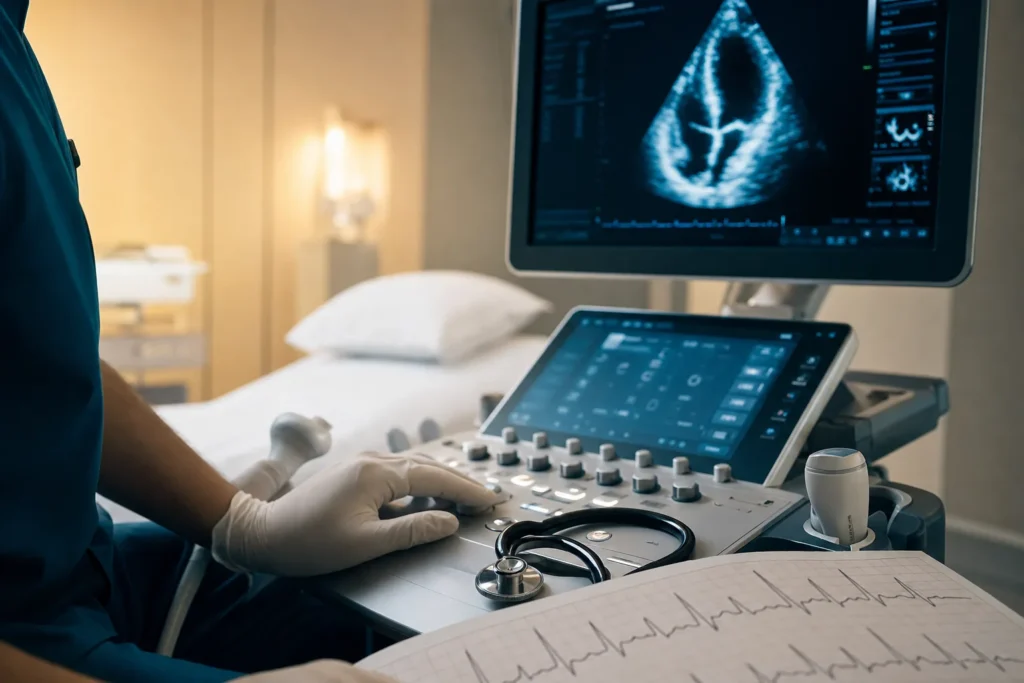
- Echocardiogram — an ultrasound scan of the heart. This is a key test because it measures the ejection fraction and shows how the chambers and valves are working.
- Electrocardiogram (ECG/EKG) — records the heart's electrical activity and can reveal rhythm problems or signs of a past heart attack.
- Chest X-ray — can show an enlarged heart or fluid in the lungs.
- Stress test, cardiac MRI or CT, and sometimes cardiac catheterization (a thin tube passed to the heart arteries) to look for narrowed arteries and measure pressures.
Doctors also "stage" heart failure. The ACC/AHA stages run from A (at risk) and B (structural change but no symptoms) to C (symptoms now or in the past) and D (advanced). The New York Heart Association (NYHA) classes I to IV describe how much symptoms limit daily activity — from no limitation (Class I) to symptoms even at rest (Class IV). Together these guide treatment and follow-up.
Treatment options
Heart failure is usually managed by a multidisciplinary team — typically a cardiologist, heart failure nurses, a pharmacist, dietitian, physiotherapist and your family doctor working together. Most people are treated with a combination of medicines, lifestyle changes and, for some, devices or surgery.
Medicines are the foundation of treatment for many people. For heart failure with a reduced ejection fraction, guideline-recommended medicines often include several of the following, introduced gradually:
- ACE inhibitors, ARBs or ARNIs — relax blood vessels and ease the heart's workload.
- Beta-blockers — slow the heart and help it work more efficiently.
- Mineralocorticoid receptor antagonists (MRAs) — help the body remove excess fluid and protect the heart.
- SGLT2 inhibitors — originally diabetes medicines, now used to protect the heart in heart failure.
- Diuretics ("water tablets") — reduce fluid build-up and ease breathlessness and swelling.
It often takes time and adjustment to find the right combination and doses, so regular review matters.
Devices and procedures for selected people include an implantable cardioverter-defibrillator (ICD) to treat dangerous rhythms, cardiac resynchronization therapy (CRT, a special pacemaker) to help the chambers beat in a coordinated way, and surgery such as valve repair or replacement or coronary bypass where appropriate. For advanced heart failure, options such as a left ventricular assist device (LVAD) or heart transplant may be considered in specialist centres.
Supportive care — including cardiac rehabilitation, dietary advice, mental-health support and, in advanced cases, palliative care to keep people comfortable — is an important part of treatment, not an afterthought.
Outlook: what to expect
Heart failure is generally a long-term condition that cannot usually be cured, although when there is a treatable cause — such as a faulty valve or an overactive thyroid — fixing it can dramatically improve or even resolve the problem.
The outlook varies a great deal from person to person. As the NHS notes, the condition tends to be unpredictable: some people stay stable for many years, while others may decline more quickly. The earlier it is found and the better the underlying causes and risk factors are managed, the more can usually be done.
Population studies show that, on average, heart failure shortens life expectancy and that survival depends strongly on age, the cause, the stage and how well treatment is followed. Any figures you read are averages across large groups of people — they are not a prediction for you as an individual, and modern medicines have improved outcomes for many. The most useful conversation about your own outlook is with your own cardiologist, who knows your test results and overall health.
What is encouraging is how much is within reach: taking medicines as prescribed, attending follow-up, watching for early warning signs, and looking after weight, salt and activity can all meaningfully improve both how you feel and how the condition behaves over time.
Living with heart failure and follow-up
Living well with heart failure is very achievable, and small daily habits make a real difference.
- Weigh yourself regularly, often each morning. A sudden gain over a day or two can mean fluid is building up — report it, as your medicines may need adjusting.
- Take your medicines as prescribed, even on days you feel well, and ask your team before stopping anything.
- Watch your salt and fluids as advised, since both affect fluid retention.
- Stay as active as you safely can. Gentle, regular activity — ideally guided by a cardiac rehabilitation programme — can boost energy, mood and sleep.
- Limit alcohol and stop smoking.
- Have recommended vaccinations (such as flu) to reduce chest infections that can worsen heart failure.
Regular follow-up appointments let your team track your ejection fraction, blood tests and symptoms and fine-tune treatment. The British Heart Foundation acknowledges that living with the uncertainty of heart failure can be hard emotionally; learning about your condition and talking openly with family and your care team can ease anxiety. Asking for psychological support is a sign of good self-care, not weakness.
Planning treatment abroad: what affects cost and how to prepare your records
If you are considering having part of your heart failure care arranged in another country, planning ahead makes everything smoother. Costs for cardiac care vary widely and depend on many factors, so a personalised estimate is far more useful than any headline figure.
Factors that affect the cost of heart failure care typically include:
- The tests needed (echocardiogram, advanced imaging, catheterization).
- Whether treatment is medicines and monitoring or a procedure such as device implantation (ICD/CRT) or valve or bypass surgery.
- The length of hospital stay and level of care required.
- Any additional conditions (diabetes, kidney disease) that need managing alongside.
- Follow-up, rehabilitation and the cost of medicines and devices themselves.
To prepare, gather your medical records: a summary from your cardiologist, recent echocardiogram and ECG reports, blood test results (including BNP/NT-proBNP and kidney function), a current medicines list with doses, details of any devices already implanted, and any imaging on disc or via a secure link. Having these translated or clearly labelled helps the receiving team plan accurately. The best next step is to request a free consultation so a specialist can review your records and give a tailored plan and estimate rather than a generic price.
Why Turkiye, and how to choose a good centre
Turkiye has become a well-known destination for cardiac care, with large hospitals that bring together cardiologists, cardiac surgeons and heart failure teams under one roof, often with international patient services that help with language, travel and scheduling.
When choosing where to be treated, focus on substance rather than slogans. Things worth verifying include:
- Accreditation — for example international quality accreditation such as JCI (Joint Commission International), and national licensing.
- A genuine multidisciplinary heart failure team, including cardiologists experienced in your specific situation and, where relevant, cardiac surgeons and electrophysiologists for devices.
- Transparent information about what is included, expected length of stay, and follow-up arrangements once you return home.
- Clear communication in a language you understand, and a written plan you can share with your doctor at home.
- Arrangements for continuity of care — how your home team will receive reports and how complications would be handled.
A reputable centre will welcome your questions, encourage a second opinion, and never pressure you. A medical concierge service can help coordinate records, appointments and logistics, but the clinical decision should always rest with qualified specialists and, ideally, in agreement with your own doctor.
Prevention and self-care
Much of what prevents heart failure also helps you live well if you already have it, because both come down to protecting the heart and keeping fluid and blood pressure in check.
- Keep blood pressure, cholesterol and blood sugar in target ranges — these are among the biggest drivers of heart failure, and treating them early matters.
- Eat a heart-healthy diet rich in vegetables, fruit, whole grains and healthy fats, and go easy on salt and processed foods.
- Stay physically active in a way that suits you; regular movement strengthens the heart and helps weight, mood and sleep.
- Maintain a healthy weight.
- Stop smoking and limit alcohol.
- Manage stress and sleep, and treat related conditions such as sleep apnoea.
If you already have heart failure, these same steps — alongside taking your medicines, weighing yourself regularly and attending follow-up — are powerful tools that you control day to day. Always check with a qualified doctor before making big changes to exercise, diet or medicines, and reach out early when something feels different. Getting a second opinion when facing major decisions is reasonable and encouraged.
Frequently asked questions
Does heart failure mean my heart is about to stop?
What is an ejection fraction, and what number is normal?
What are the warning signs I should act on?
Can heart failure be cured?
How is heart failure diagnosed?
What medicines are used for heart failure?
Will I need a device or surgery?
What is the outlook for someone with heart failure?
Can I exercise and travel with heart failure?
How do I prepare my records for treatment abroad?
What should I look for in a heart centre in Turkiye?
This article is for general information only and is not medical advice. Always consult a qualified doctor about your individual case.
Considering this procedure?
Send us your photos and questions. A BergemHealth coordinator and a department-head specialist will review your case and reply with honest, personalised guidance — no obligation.
Free consultation