Epilepsy
Epilepsy is one of the most common conditions of the brain, affecting around 50 million people worldwide. A diagnosis can feel frightening at first, but for most people seizures can be well controlled and a full, active life is very much possible. This guide explains, in plain language, what epilepsy is, why it happens, how doctors diagnose and treat it, and how to prepare if you are considering specialist neurology care in Turkiye.
What epilepsy is
Epilepsy is a long-term condition of the brain that causes repeated seizures. A seizure is a short burst of unusual electrical activity in the brain. Brain cells (called neurons) normally communicate using tiny, well-organised electrical signals. During a seizure, a group of these cells fires together in a sudden, disorganised way, and that brief "electrical storm" temporarily changes how a part of the brain works. Depending on which area is involved, this can affect movement, sensation, awareness, mood or behaviour.
One seizure on its own does not mean a person has epilepsy. Doctors usually diagnose epilepsy when someone has had two or more unprovoked seizures (seizures not caused by a clear, reversible trigger such as a very high fever or low blood sugar) more than 24 hours apart, or after one seizure when tests show a high chance of more happening. Seizures themselves are common; many things, from a serious illness to extreme sleep deprivation, can provoke a single seizure. Epilepsy specifically refers to an ongoing tendency to have them.
Epilepsy is common. Around 50 million people worldwide live with it, making it one of the most common serious neurological (nervous-system) conditions. It affects people of every age, background and gender. Many people picture only dramatic convulsions, but in reality seizures take many forms, some so subtle that they can be mistaken for daydreaming or confusion.
Types of epilepsy and seizures
Doctors group seizures by where in the brain they begin. Understanding the type matters, because it guides which treatment is most likely to help.
Focal seizures (also called partial seizures) start in one area of the brain. There are two kinds:
- Focal aware seizures: the person stays conscious and aware. They may notice a strange taste or smell, a rising feeling in the stomach, tingling, a sense of deja vu, or sudden emotion. These warning sensations are sometimes called an aura.
- Focal impaired awareness seizures: awareness is reduced or lost. The person may seem distant or confused, stare, or make repeated movements such as lip-smacking, fiddling or wandering, with no memory of it afterwards.
Generalised seizures involve both sides of the brain from the start, and usually affect awareness. Main types include:
- Tonic-clonic (once called "grand mal"): the body stiffens, then jerks rhythmically; the person loses consciousness and may fall. This is the type most people recognise.
- Absence (once called "petit mal"): brief blank spells, lasting a few seconds, common in children and easily mistaken for inattention.
- Myoclonic: sudden, brief jerks of an arm, leg or the whole body.
- Tonic: muscles suddenly stiffen, which can cause a fall.
- Atonic ("drop attacks"): muscles suddenly go floppy, causing a sudden fall.
- Clonic: rhythmic jerking movements.
When it is not clear where a seizure began, doctors call it unknown onset. Some patterns of epilepsy that begin in childhood and have a typical age of onset, seizure type and test findings are grouped into epilepsy syndromes, which can help predict the likely course and best treatment.
Causes and risk factors
It is important to know that in roughly half of all people with epilepsy, no clear cause is ever found. This is normal and does not mean the condition is being missed or mismanaged. When a cause is identified, it usually falls into one of these groups:
- Genetic factors: some forms of epilepsy run in families or are linked to particular genes that affect how brain cells signal. Having a family history does not mean a person will definitely develop epilepsy.
- Structural changes in the brain: a stroke, a brain tumour, scarring, or a difference in how the brain formed before birth can create an area prone to seizures.
- Head injury: a serious blow to the head can lead to epilepsy, sometimes months or years later.
- Infections: illnesses such as meningitis or encephalitis (infections affecting the brain or its lining). Worldwide, a parasitic infection called neurocysticercosis is a leading preventable cause.
- Problems around birth: lack of oxygen or other complications during birth.
- Other conditions: some metabolic or autoimmune disorders, and brain changes linked to conditions such as Alzheimer's disease in older adults.
Known risk factors include a family history of epilepsy, previous serious head injury, stroke, brain infection, and certain developmental conditions. Stroke is a particularly common cause of new epilepsy in older people. Having a risk factor does not mean a person will develop epilepsy, and many people with epilepsy have none of them.
Signs, symptoms and when to see a doctor
Because seizures can affect any part of the brain, symptoms vary enormously. They may include:
- Becoming stiff, or suddenly going floppy and falling
- Jerking or shaking movements you cannot control
- Brief blank or staring spells with loss of awareness
- Strange sensations such as an unusual smell or taste, tingling, or a rising feeling in the stomach
- Sudden feelings of fear, deja vu or confusion
- Repetitive movements such as lip-smacking, chewing or fiddling
- Temporary loss of consciousness, sometimes with loss of bladder control or biting the tongue
Most seizures last only seconds to a couple of minutes and stop on their own. Afterwards a person may feel tired, confused or have a headache for a while; this recovery period is normal.
When to seek emergency help: Call emergency services if a seizure lasts longer than 5 minutes, if one seizure follows another without the person recovering in between, if the person is injured or has trouble breathing, or if it is their first-ever seizure. A seizure that does not stop, called status epilepticus, is a medical emergency and needs immediate treatment.
When to see a doctor (non-emergency): Make an appointment if you have had a seizure for the first time and recovered, if you notice blank spells, unexplained jerks, or odd repeated sensations, or if you have epilepsy and your seizures change in type or frequency. A clear description from someone who saw the event is extremely helpful, so bring a witness or their account if you can.
Screening and early detection
There is no routine screening test for epilepsy in the general population, in the way there is for some cancers. Epilepsy cannot be detected before symptoms appear, and there is no blood test or scan that everyone should have to "check for" it.
Instead, "early detection" means recognising seizures and seeking medical advice promptly. Subtle seizures, such as brief staring spells in children or short episodes of confusion in adults, are easy to dismiss, so being aware that these can be seizures is valuable. The single most useful thing you can do is to describe events accurately to a doctor and, where possible, have someone record what happens, even on a phone, since video of an event can help a specialist a great deal.
People who have a known higher risk, for example after a significant head injury, stroke or brain infection, should be alert to possible seizure symptoms and mention any unusual episodes to their doctor. Getting a proper assessment after a first suspected seizure is the key step, because starting the right treatment early can reduce the chance of further seizures and related injury.
How epilepsy is diagnosed
Diagnosis begins with a careful history: the doctor (usually a neurologist, a specialist in conditions of the brain and nervous system) asks what happened before, during and after the episode, and ideally hears from someone who witnessed it. This account is often the most important part of the diagnosis, because seizures are usually over by the time a patient reaches a clinic.
Tests are then used to support the diagnosis and look for a cause:
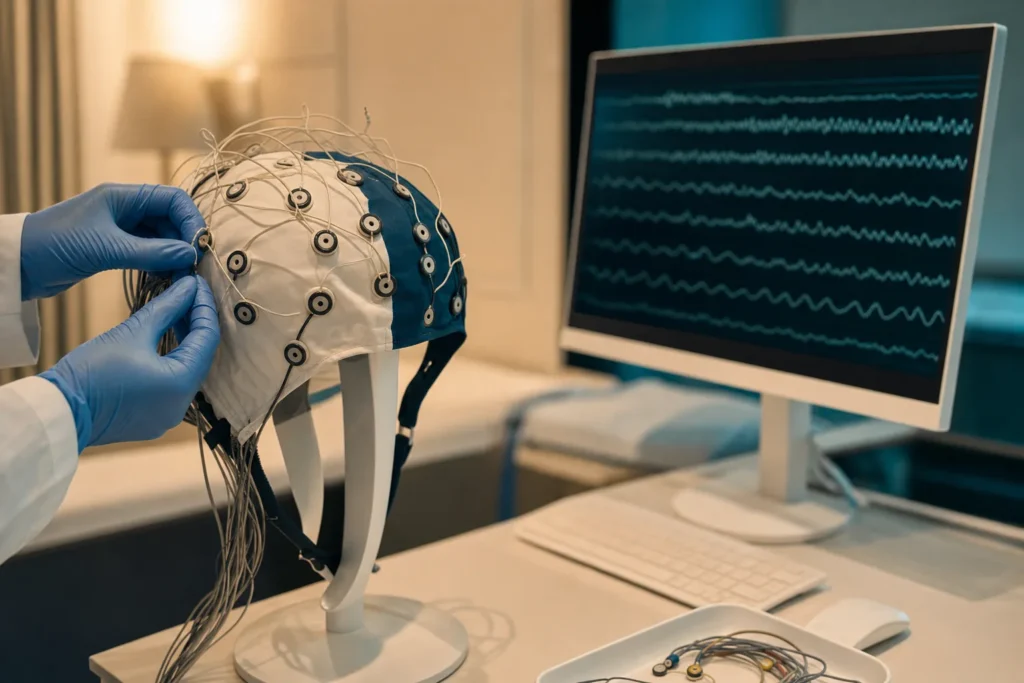
- EEG (electroencephalogram): small sensors on the scalp record the brain's electrical activity and can pick up patterns linked to epilepsy. A normal EEG does not rule out epilepsy, and an unusual one alone does not confirm it; results are read alongside the clinical story.
- Brain imaging (MRI or CT scan): detailed pictures of the brain that can reveal a structural cause such as scarring, a malformation, the effects of a stroke, or a tumour. MRI gives the most detail.
- Blood tests: to check for infections, metabolic problems, or other conditions that can cause seizures.
- ECG (heart trace): sometimes used because some heart-rhythm problems can cause fainting or collapse that mimics a seizure.
- Genetic testing: considered in some cases, particularly certain epilepsies that begin in childhood.
Unlike cancer, epilepsy is not "staged". Instead, doctors classify the seizure type, identify any epilepsy syndrome, and look for an underlying cause, because this is what guides the choice of treatment. Sometimes the diagnosis becomes clear only over time, as the pattern of events emerges.
Treatment options
The aim of treatment is to stop seizures, or reduce them as much as possible, while keeping side effects low. Care is usually led by a neurologist, often working with a multidisciplinary team that may include epilepsy nurses, neurosurgeons, neuropsychologists, pharmacists and, for children, paediatric specialists.
Anti-seizure medicines (also called anti-epileptic drugs) are the main treatment and the first step for almost everyone. They do not cure epilepsy, but they reduce the brain's tendency to have seizures. There are many different medicines, and the choice depends on the seizure type, age, sex, other health conditions and possible side effects. It can take time and some adjustment to find the right medicine and dose. According to the World Health Organization, up to 70% of people with epilepsy could become seizure-free with the appropriate use of anti-seizure medicines. Medicines should never be stopped suddenly without medical advice, as this can trigger seizures.
When seizures continue despite trying two suitable medicines at proper doses, the epilepsy is described as drug-resistant (or refractory). At this point a specialist epilepsy centre can assess whether other treatments may help:
- Epilepsy surgery: if seizures reliably start in one well-defined, safe-to-treat area, an operation to remove or disconnect that area may greatly reduce or stop seizures. Newer, less invasive techniques such as laser ablation are available in some centres.
- Neurostimulation devices: these use mild electrical pulses to calm seizure activity. They include vagus nerve stimulation (a small device placed under the skin of the chest), and, in selected cases, responsive neurostimulation or deep brain stimulation.
- Dietary therapy: a strict, medically supervised ketogenic diet (high in fat, very low in carbohydrate) can reduce seizures in some people, especially children with certain hard-to-treat epilepsies.
People are also given advice on emergency or "rescue" treatment for prolonged seizures, and on managing triggers. The right combination is highly individual, which is why specialist assessment matters.
Outlook: what to expect
For most people, the outlook is reassuring. Epilepsy is generally a manageable long-term condition, and many people lead full lives with work, relationships, travel and family. As noted above, up to 70% of people can become seizure-free with the right medicines, and some children and adults eventually come off medication after a long seizure-free period, always under medical guidance.
For those whose seizures do not fully respond to the first medicines, additional treatments at a specialist centre can still bring major improvement. The course of epilepsy varies a great deal from person to person, and these figures describe groups of people, not a prediction for any single individual; your own outlook depends on your seizure type, cause and how you respond to treatment, which your doctor can discuss with you.
It is honest to mention that epilepsy carries some risks that careful management aims to reduce. The risk of premature death is somewhat higher than in the general population, often related to accidents during seizures, prolonged seizures (status epilepticus), or an uncommon event called SUDEP (sudden unexpected death in epilepsy). SUDEP is rare, affecting roughly 1 in 1,000 adults with epilepsy each year, and the risk is mainly linked to frequent tonic-clonic seizures, especially during sleep, and to missed medication. The most effective way to lower these risks is to get seizures as well controlled as possible and take medicines as prescribed, which is exactly what good specialist care is designed to achieve. Your neurologist can talk through SUDEP and practical steps to reduce risk; you should feel able to ask.
Living with epilepsy and follow-up
Living well with epilepsy is largely about steady, sensible routines and good support. Helpful day-to-day measures include:
- Taking medication consistently at the same times each day; missed doses are a common, avoidable cause of breakthrough seizures.
- Keeping a seizure diary to record when seizures happen and any possible triggers, which helps you and your doctor fine-tune treatment.
- Knowing your triggers, which can include lack of sleep, stress, alcohol, missed meals, illness with fever, and, for a minority, flashing lights.
- Prioritising sleep, since being overtired is one of the most common triggers.
- Sensible safety steps, such as care around water, heights and certain machinery, and adapting the home if needed. Carrying medical identification can help others respond correctly.
Practical issues matter too. Many countries have driving rules that require a seizure-free period before driving; check the regulations where you live. Most jobs, sports and activities remain open to people with epilepsy, sometimes with simple precautions. Pregnancy is usually safe and successful but should be planned with your doctor, as some medicines need review beforehand.
Follow-up is ongoing rather than a single course of treatment. Regular reviews let your team check how well seizures are controlled, adjust medicines, monitor side effects, and support your wider wellbeing, including mood, since anxiety and low mood are common and very treatable alongside epilepsy. Telling family, friends or colleagues what to do during a seizure (stay calm, protect from injury, time the seizure, do not put anything in the mouth, and call for help if it lasts over 5 minutes) can make everyday life safer and less worrying for everyone.
Planning treatment abroad: what affects cost and how to prepare
If you are considering specialist epilepsy assessment or treatment abroad, it helps to understand what shapes the overall cost so you can plan realistically. We do not list prices here because every situation is different, and an honest estimate can only be given once a specialist has reviewed your records. The main factors include:
- What you actually need: a diagnostic work-up (such as MRI and EEG, or longer video-EEG monitoring) costs very differently from medical management, which differs again from epilepsy surgery or a neurostimulation device.
- The extent of investigations: drug-resistant epilepsy often requires more detailed pre-surgical testing, which affects time and cost.
- Length of stay and whether monitoring or an operation requires inpatient care.
- The medical team and facility, including the seniority of specialists and the type of hospital.
- Medicines and follow-up, including any rescue medication and review appointments.
- Travel and accommodation for you and a companion, and any interpreting or coordination services.
To prepare, gather your medical records: a list of all seizures with dates and descriptions (a seizure diary is ideal), every anti-seizure medicine you have tried with doses and effects, copies of previous EEG and MRI/CT reports and the images themselves where possible, and a summary letter from your current doctor. Video of a typical seizure can be very valuable. Having these ready allows a specialist to review your case properly and provide a clear, personalised plan and estimate. Because individual needs vary so much, the most reliable next step is to request a free consultation so a specialist can review your records and outline what is appropriate for you.
Why Turkiye, and how to choose a good centre
Turkiye has become a well-established destination for international patients seeking neurology and neurosurgery care, with experienced specialist teams, modern hospitals and dedicated international patient services. The country regulates health tourism through its Ministry of Health, and facilities that treat international patients are expected to hold a Health Tourism Authorisation Certificate, which sets requirements around interpreter services, international patient coordination and informed consent. Turkiye is also home to a large number of hospitals accredited by Joint Commission International (JCI), an internationally recognised standard for quality and patient safety.
Accreditation and authorisation are useful signals, but it is wise to verify a few things for yourself before committing. When choosing a centre for epilepsy care, consider asking about:
- Specialist expertise: whether the team includes neurologists with a specific focus on epilepsy, and, where surgery is considered, neurosurgeons and a dedicated epilepsy or video-EEG monitoring unit.
- The multidisciplinary team: access to epilepsy nurses, neuropsychology, neuroradiology and, for children, paediatric neurology.
- Accreditation: confirmation of JCI accreditation and the Health Tourism Authorisation Certificate.
- Clear, written information: a treatment plan, consent documents in a language you understand, and transparent details of what is included.
- Continuity of care: how follow-up will work once you return home, and how your local doctor will receive your records and any changes to medication.
- Communication: interpreting support and a named coordinator you can reach with questions.
Take your time, ask questions, and make sure you feel comfortable with the answers. A reputable centre will welcome these questions and give you clear, unhurried information.
Reducing risk and self-care
While many cases of epilepsy cannot be prevented, you can take meaningful steps to lower the chance of some causes and to protect your brain and your seizure control:
- Protect your head: wear seatbelts and appropriate helmets, and reduce fall risks, since head injury is a preventable cause of epilepsy.
- Look after your heart and blood vessels: managing blood pressure, not smoking, staying active and eating well lowers the risk of stroke, a leading cause of new epilepsy in older adults.
- Reduce infection risk: vaccination, good food hygiene and prompt treatment of brain infections help prevent infection-related seizures.
- Care in pregnancy and around birth: good antenatal care reduces birth complications that can lead to epilepsy.
If you already have epilepsy, self-care focuses on staying seizure-free and safe: take medicines exactly as prescribed and never stop them abruptly, keep regular sleep, manage stress, be cautious with alcohol, identify and avoid your personal triggers, and attend follow-up appointments. Looking after your mental health matters too, so reach out if you feel low or anxious, as support is available and effective.
Finally, if your seizures are not fully controlled, it is reasonable to ask your doctor about a referral to a specialist epilepsy centre or to seek a second opinion. Drug-resistant epilepsy in particular benefits from expert assessment, and getting another informed view is a normal, sensible part of managing a long-term condition.
Frequently asked questions
Is epilepsy curable?
Does having one seizure mean I have epilepsy?
What should I do if I see someone having a seizure?
What causes epilepsy?
Is epilepsy inherited?
Can people with epilepsy live a normal life?
What is drug-resistant epilepsy?
What is SUDEP and how can the risk be lowered?
Will I need brain surgery for epilepsy?
How is epilepsy diagnosed?
What information should I bring when planning treatment abroad?
Why might I consider epilepsy care in Turkiye?
This article is for general information only and is not medical advice. Always consult a qualified doctor about your individual case.
Considering this procedure?
Send us your photos and questions. A BergemHealth coordinator and a department-head specialist will review your case and reply with honest, personalised guidance — no obligation.
Free consultation