Fracture & revision surgery
A broken bone or a worn-out joint implant can stop your life in its tracks. This guide explains, in plain words, how surgeons fix fractures and redo previous orthopedic operations, what recovery really looks like, and how to choose a safe clinic if you are considering treatment in Turkiye.
- Anaesthesia
- General anaesthesia, or regional (spinal/nerve block) with sedation, depending on the bone and procedure.
- Duration
- Roughly 1-3 hours for most fracture fixation; revision joint surgery often takes several hours.
- Recovery
- Bones typically heal in 6-12 weeks; full recovery and physiotherapy can take several months to a year.
- Hospital stay
- Day case to 1-2 nights for many fractures; several days for revision joint replacement.
What it is
Fracture surgery and revision surgery are two closely related parts of orthopedics, the branch of medicine that deals with bones, joints, muscles and tendons. They often involve the same tools and the same surgeons, which is why hospitals usually group them together.
A fracture is simply the medical word for a broken bone. Many breaks heal well in a plaster cast. But when the pieces are out of place, broken into several fragments, or poking through the skin, a cast is not enough. The surgeon then operates to put the bone back into its correct shape (this is called reduction) and hold it there with metal implants while it knits back together.
Revision surgery means an operation to redo or repair a previous orthopedic procedure that has not worked as hoped. The most common example is a worn-out or loosened artificial hip or knee that needs to be partly or fully replaced. "Revision" can also mean fixing a fracture that failed to heal (called a nonunion), correcting a bone that healed crooked (a malunion), or removing and replacing metalwork that has loosened or become infected.
In short: fracture surgery puts a broken bone right the first time, and revision surgery is the planned, more complex operation to set things right when an earlier repair or implant has run into trouble.
Who is a good candidate
You may need fracture surgery if an X-ray or scan shows that your broken bone is:
- Displaced - the broken ends have shifted out of line and will not heal straight on their own.
- Comminuted - shattered into three or more pieces.
- Open (compound) - the bone has broken through the skin, which raises the risk of infection and usually needs urgent surgery.
- Inside or close to a joint, where even a small step in the bone surface can cause long-term pain and arthritis.
Revision joint surgery is considered when an existing implant causes problems such as ongoing pain, the joint loosening from the bone, the plastic spacer wearing out, repeated dislocations, instability, stiffness, infection, or a new break around the implant (a periprosthetic fracture).
Who may need to avoid or delay surgery, or proceed with extra care: people with an active untreated infection elsewhere in the body, very poorly controlled diabetes, severe heart or lung disease that makes anaesthesia risky, or uncontrolled bleeding disorders. Smoking and heavy alcohol use slow bone healing and raise the chance of complications, so surgeons often ask you to stop well before the operation. The right plan is always decided case by case after examination and imaging.
Types & techniques
Surgeons choose the technique based on which bone is broken, the pattern of the break, your age, bone quality and general health.
For fractures:
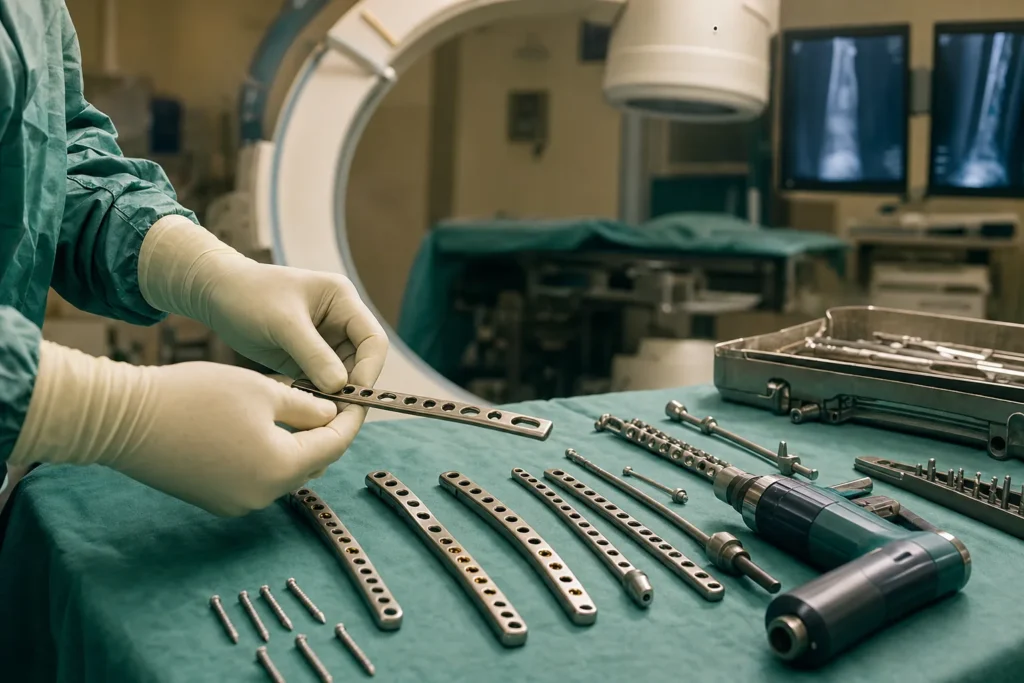
- Open reduction and internal fixation (ORIF) - the surgeon opens the skin, lines the pieces back up, and fixes them in place with metal implants left inside the body.
- Plates and screws - a metal plate acts like an internal splint and is held to the bone with screws. Screws are the most commonly used implant of all.
- Intramedullary nail (rod) - a metal rod slid down the hollow centre of a long bone such as the thigh (femur) or shin (tibia), locked with screws at each end to stop the bone shortening or twisting.
- Wires and pins - used for small fragments, such as in the hand, foot or in children, sometimes alongside other implants.
- External fixation - pins or screws go into the bone above and below the break and connect to a frame outside the skin. It is often used when the soft tissue is badly damaged, or as a temporary measure until the patient is well enough for final surgery.
Implants are usually made of titanium or stainless steel, which the body tolerates well. Tell your surgeon if you have a nickel allergy.
For revision: revision joint replacement uses specialised implants, often with longer stems for extra grip, plus metal augments or bone grafts (your own bone, donor bone, or a substitute) to rebuild areas where bone has been lost. When infection is involved, surgeons may use a two-stage approach: remove the old implant, place a temporary antibiotic spacer for several weeks, then implant the new joint.
How it is done
Anaesthesia. Most fracture and revision operations are done under general anaesthesia (you are fully asleep) or regional anaesthesia such as a spinal injection or nerve block that numbs the limb, often combined with sedation so you are relaxed and comfortable. The anaesthetist chooses the safest option for you.
The steps, in plain terms:
- You are positioned and the skin is cleaned and sterilised.
- The surgeon makes an incision to reach the bone, or in some cases works through small cuts using live X-ray to guide the implants.
- The bone fragments are repositioned into their normal alignment (reduction).
- Plates, screws, a rod, pins or an external frame are fitted to hold everything steady.
- For revision, the old implant or hardware is carefully removed first - a slow, painstaking step, especially if bone cement has to be chipped out - then any bone loss is rebuilt and the new components are fitted.
- The wound is closed and a dressing, and sometimes a splint, is applied.
How long it takes. A straightforward fracture fixation often takes about one to three hours. Complex fractures and revision joint replacements are longer, more demanding operations that frequently take several hours because of the extra planning, hardware removal and bone reconstruction involved.
Recovery, step by step
Recovery depends heavily on which bone or joint was treated, but the general path is similar.
- First days. Expect pain that is managed with medication, swelling, and a dressing or splint. Many simple fractures are treated as a day case or with one to two nights in hospital; revision joint replacement usually means several days as an inpatient.
- First weeks. You may need a cast, brace, sling, crutches, a walker or a cane. Your team will tell you how much weight you can safely put on the limb - sometimes none at first. Keeping the limb elevated helps reduce swelling.
- Physiotherapy. Gentle, guided movement often starts early to prevent stiffness and rebuild strength. After a knee revision, for example, a key early goal is regaining about 90 degrees of bend.
- Bone healing. Most broken bones knit in roughly 6 to 12 weeks. Small bones such as fingers may heal in 3 to 4 weeks, while a shin (tibia) fracture commonly takes 4 to 6 months, and severe or open fractures can take a year or more.
- Follow-up. X-rays at intervals check that the bone is healing in the right position. Stitches or clips are usually removed within a couple of weeks. Most people need help at home for several days to several weeks.
Healing is slower if you smoke, have diabetes, low vitamin D, poor nutrition or take certain anti-inflammatory medicines, so following your team's advice closely really does make a difference.
Risks & possible complications
These are generally safe, well-established operations, but no surgery is risk-free. Possible complications include:
- Infection - of the wound or the bone (osteomyelitis). Infection risk is higher in revision surgery than in a first-time operation.
- Blood clots - in the leg veins (deep vein thrombosis) or, rarely, the lungs (pulmonary embolism). Risk is highest in the days and weeks after surgery.
- Nonunion or malunion - the bone fails to heal, or heals in a crooked position.
- Hardware problems - implants can loosen, break, irritate nearby tissue, or occasionally need removal later.
- Nerve or blood-vessel injury near the operation site.
- Stiffness or reduced range of movement, especially after joint surgery.
- For joint revision specifically - dislocation, a difference in leg length, and a somewhat higher overall complication rate than primary (first-time) replacement.
- Compartment syndrome - a rare but urgent build-up of pressure in a limb that needs immediate treatment.
Your surgeon should explain which risks are most relevant to your specific case before you sign the consent form.
Results & how long they last
For most people, the results are good. A well-fixed fracture allows the bone to heal in the correct shape and restores function, and many return to normal or near-normal activity. As an indication of outcomes, studies cited by Cleveland Clinic found that around 75% of people who had ORIF for a broken thigh bone had few or no long-term complications.
Metal implants used for fractures often stay in place permanently and cause no trouble. They are only removed if they become painful, prominent, loose or infected - and when removal is chosen, it is usually considered around a year or more after the bone has fully healed.
For revision joint replacement, most patients gain lasting pain relief and better function. However, because the bone and soft tissues have already been operated on once, some people continue to have some pain or stiffness, and a revised joint may not last as long as a first replacement. How long any implant lasts depends on your age, weight, activity level and bone quality - which is why surgeons advise sensible, lower-impact activity to protect the result.
Costs
Cost varies enormously because "fracture and revision surgery" covers everything from pinning a finger to a full, multi-hour revision hip replacement with bone grafting. As a very rough guide, prices in Turkiye for international patients often fall somewhere between around 2,500 EUR for a straightforward single-bone fracture fixation and 20,000 EUR or more for a complex revision joint replacement with specialised implants.
What changes the price:
- Which bone or joint is involved, and how complex the break or revision is.
- The type and number of implants (a standard plate costs far less than custom revision components or augments).
- Whether bone grafting, a two-stage infection treatment, or extra reconstruction is needed.
- Length of hospital stay, intensive-care needs, and physiotherapy.
- The surgeon's experience and the hospital's accreditation level.
- Pre-operative scans, anaesthesia, medication and follow-up X-rays.
These figures are indicative ranges only. They are not a quote. Actual cost varies by case, surgeon and clinic. Always ask for a written, itemised quotation that states exactly what is and is not included before you commit.
Why people travel to Turkiye & how to choose a safe clinic
Turkiye has become a popular destination for orthopedic care because of well-equipped private hospitals, experienced surgeons and prices that are often lower than in Western Europe, North America or the Gulf - frequently with short waiting times and all-inclusive packages that bundle the surgery, hospital stay and transfers.
Lower price should never mean lower standards. Before you book, verify the following:
- Hospital accreditation. Look for international accreditation such as JCI (Joint Commission International) and proper Turkish Ministry of Health licensing.
- Surgeon credentials. Confirm the surgeon is a board-certified orthopedic specialist, ideally with a sub-specialty in trauma or joint revision, and ask how many cases like yours they perform each year.
- A clear, written plan. A reputable clinic gives you a named surgeon, an itemised quote, and an honest discussion of risks - not vague promises or pressure to decide quickly.
- Realistic claims. Be cautious of anyone promising a "guaranteed" result or using "best/safest" superlatives; good surgeons talk in probabilities, not guarantees.
- Aftercare and communication. Check who looks after you if a complication appears after you fly home, and whether records and X-rays will be shared with your doctor at home.
A trustworthy concierge service or clinic will happily answer all of these questions in writing.
How to prepare & what to ask in your consultation
To prepare: gather your imaging (X-rays, CT or MRI), a list of your medicines and allergies, and the full history of any previous operations on the same bone or joint - this is essential for revision planning. Stop smoking as early as possible, as it directly slows bone healing. Tell the team about blood thinners, diabetes, heart or lung conditions, and any nickel allergy. You may need blood tests and a fitness-for-anaesthesia check beforehand.
Useful questions to ask your surgeon:
- What exactly is wrong, and what would happen if I did nothing or waited?
- Which technique do you recommend for me, and why?
- What kind of anaesthesia will I have?
- How many of these procedures do you do each year, and what are your complication rates?
- What are the main risks in my specific case?
- How long is the hospital stay, and how soon can I bear weight or move the joint?
- Will I need the metalwork removed later?
- What does the written quote include - and what is excluded?
- What is the plan if a complication happens after I travel home?
Aftercare & travelling for treatment
After surgery you will have a recovery plan covering wound care, pain relief, weight-bearing limits, exercises and follow-up X-rays. Take blood-clot prevention seriously: this may include blood-thinning medication, compression stockings and early, gentle movement as advised.
When is it safe to fly? Flying soon after surgery raises the risk of a blood clot, and that risk is already highest in the first days and weeks afterward. Many orthopedic surgeons suggest avoiding air travel for at least two weeks after surgery, and waiting roughly four to six weeks before longer flights - particularly after lower-limb or joint surgery. The right timing depends on your operation and health, so always get personal clearance from your surgeon before booking a flight home.
During the flight, reduce clot risk by walking when you safely can, doing regular ankle-pumping exercises (flexing your foot up and down) in your seat at least once an hour, staying well hydrated, and wearing any compression stockings you have been given.
Practical travel tips: arrange enough time in the country for your post-op checks and stitch removal before flying; carry a copy of your operation notes, implant details and X-rays; plan for help with luggage and getting around; and make sure you know exactly who to contact - and how - if you notice signs of infection (increasing redness, warmth, discharge or fever) or a possible clot (a swollen, painful calf, or sudden chest pain or breathlessness, which needs emergency care).
Frequently asked questions
What is the difference between fracture surgery and revision surgery?
Do all broken bones need surgery?
How long does a broken bone take to heal after surgery?
Why would I need revision joint replacement?
What type of anaesthesia is used?
Will the metal plates and screws need to be removed later?
Is revision surgery riskier than the first operation?
How soon can I fly home after surgery?
What can I do to lower my risk of a blood clot when travelling?
What makes the cost of fracture or revision surgery go up or down?
How do I check that a clinic and surgeon in Turkiye are safe?
What is a nonunion, and how is it treated?
This article is for general information only and is not medical advice. Always consult a qualified doctor about your individual case.
Considering this procedure?
Send us your photos and questions. A BergemHealth coordinator and a department-head specialist will review your case and reply with honest, personalised guidance — no obligation.
Free consultation